
What Are Ear Correctors?
The term “ear corrector” is broad and can be misleading. In essence, it refers to any device or method designed to alter the shape or position of the ear. However, the effectiveness, mechanism, and permanence of these correctors vary dramatically based on their type and, most importantly, the age of the user. From medical-grade solutions for newborns to consumer products for adults, the world of ear correctors is diverse.
This article will demystify these devices, exploring everything from infant ear molding systems to over-the-counter products like ear corrector tape, ear corrector stickers, and ear corrector clips.
Two Distinct Worlds: Medical Devices vs. Cosmetic Aids
The first and most critical distinction to make is between two categories:
Medical Correctors: These are clinically proven devices used under professional guidance, almost exclusively for newborns and infants. Examples include a Newborn ear corrector or Infant ear corrector system for infant ear molding.
Cosmetic/Consumer Correctors: These are non-medical, typically adhesive or clip-based products marketed for temporary use. They are often advertised as ear correctors for adults and include ear corrector stickers, tape, and clips.
Understanding this divide is key to setting realistic expectations.
Medical Ear Correctors: A Miracle of Early Intervention
For babies, an ear corrector is a legitimate medical tool with an incredibly high success rate.
What are they?
A medical ear corrector for babies is a non-surgical splinting system. It is not a simple piece of tape. These systems, such as the EarWell™ or EarBuddies™ kits, are sophisticated and often consist of:
A soft, malleable plastic or metal framework.
A silicone shell or cradle that holds the ear in the desired shape.
Medical-grade adhesive ear corrector stickers or tape to secure the system in place.
A retention base that attaches to the cheek or side of the head.
How do they work?
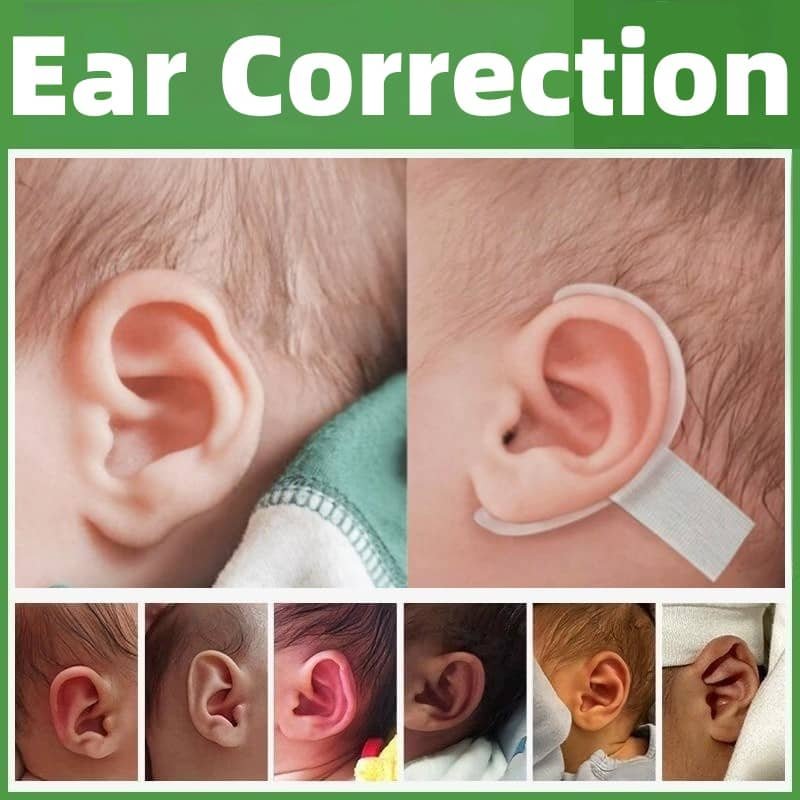
They leverage a biological golden window. In the first few weeks of life, a newborn’s cartilage is soft and pliable due to high levels of maternal estrogen. An Infant ear corrector system applies gentle, constant pressure to mold this soft cartilage into a more typical shape. The process, known as infant ear molding, typically takes 4-6 weeks.
What do they treat?
These systems are highly effective for a range of ear deformity newborn conditions, including:
Protruding ear / Prominent ear / Stick Out Ear
Lop ear and lop ear deformity correction
Cup ear and cup ear deformity correction
Constricted ear
Stahl’s Ear (characterized by an extra fold)
Cryptotia (“hidden ear”)
Earlobe deformities
When applied by a specialist within the first two weeks of life, infant ear correction has a success rate of over 90%. This is a true, permanent correction that can prevent the need for future surgery.
Consumer Ear Correctors for Adults: Managing Expectations
For adults and older children, the term ear corrector takes on a different, less permanent meaning. Since ear cartilage hardens and loses its plasticity within the first few months of life, no external device can permanently reshape it without surgery.
Consumer products are essentially cosmetic concealment tools. The main types are:
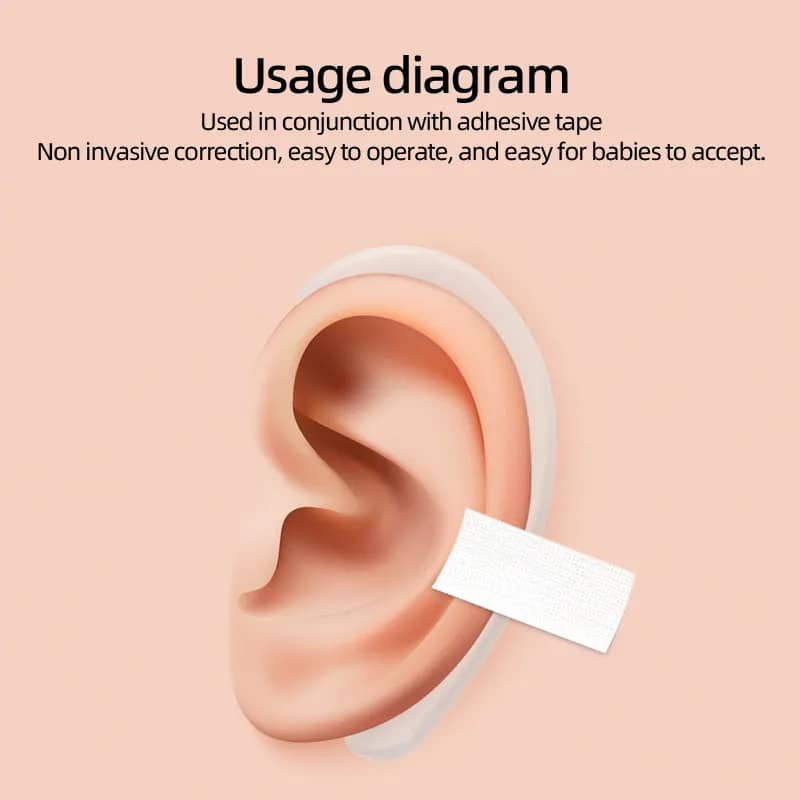
1. Ear Corrector Tape / Stickers
What are they? These are double-sided adhesive strips. One side sticks to the back of the ear (the antihelix or conchal bowl) and the other to the scalp, physically pulling the ear closer to the head.
Reality Check: They offer a temporary solution. The effect lasts only as long as the tape is attached. They are not designed for cup ear correction or fixing Stahl’s Ear; they only address protrusion. They can cause skin irritation, are not waterproof, and can be visible if not carefully placed.
2. Ear Corrector Clip
What is it? A small, often plastic, clip that attaches to the helical rim (the outer edge) of the ear, applying pressure to bend it backward.
Reality Check: Like tape, its effects are temporary. It can be uncomfortable, cause pain or pinching, and may even damage the skin or cartilage with prolonged use. It is not a viable long-term or permanent solution.
The Verdict for Adults:
Products marketed as ear correctors for adults are misnamed. A more accurate term would be “ear concealer” or “ear holder.” They can be useful for a special event, photo, or when wearing a specific hairstyle, but they should not be expected to provide any lasting change. For a permanent protruding ear corrector, otoplasty (surgical ear pinning) is the only effective option.
Choosing the Right Path: A Summary
| Feature | Medical Infant Corrector | Consumer Adult “Corrector” |
|---|---|---|
| Target Age | Newborns (0-8 weeks) | Adults & Older Children |
| Mechanism | Molds soft cartilage | Adheres to skin or clips to cartilage |
| Permanence | Permanent correction | Temporary concealment |
| Effectiveness | High (>90% success) | Low (cosmetic only) |
| Professional Role | Applied & monitored by a doctor | Self-applied |
| Best For | Infant ear deformity, cup ear, lop ear, Stahl’s Ear | Temporary confidence boost for prominent ears |
Conclusion: A Term with Two Meanings
So, what are ear correctors? The answer has two parts.
For infants, an ear corrector is a life-changing medical device. It represents a safe, non-invasive, and highly effective method to permanently reshape ears and correct conditions like constricted ear, cryptotia, and protruding ears, saving the child from potential future surgery and psychological distress.
For adults, an ear corrector is a cosmetic aid. Products like ear corrector tape, stickers, and clips can only offer a temporary illusion of less prominent ears. They are not solutions for complex deformities and provide no permanent alteration.
The key is to understand this crucial distinction. If you are a parent of a newborn with a suspected infant ear deformity, act quickly and consult a medical professional. If you are an adult seeking change, be realistic about the temporary nature of consumer products and consult a plastic surgeon to discuss the permanent, surgical solution that otoplasty provides.